


Aligning the bony nasal vault in rhinoplasty
The bony nasal vault represents a complex three dimensional structure. With a widely divergent spectrum of nasal bony deformities, use of a single technique will often result in inconsistent results. Recognition of the underlying geometric osseous form allows the surgeon to utilize a ratiocinative approach in addressing deformities of the upper one third of the nose.
Nasal width anatomy, aesthetics
Nasal osteotomies are controlled fractures of the nasal bones and/or adjacent maxillary processes. The nasal bones vary in thickness from person to person. The average thickness along a lateral osteotomy track was determined to be 2.47 mm in male patients and 2.29 mm in female patients, with statistically age-related decrease in bony thickness for male patients without a corresponding observation in female patients. (1) Citardi and associates reviewed CT scan data and found that nasal bone thickness at the level of lateral osteotomy was 2.39 +/- 0.68 (mean + SD) mm, while nasal bone thickness at the level of intermediate osteotomy was 1.18 + 0.30 mm. (2)
The relationship of the nasal bones and the nasolacrimal duct system is under appreciated. An approximation of the nasolacrimal canal can be determined by drawing a line from the lacrimal fossa to the anterior attachment of the inferior turbinate. (3) The distance of the nasolacrimal duct usually lies deep within the maxilla, but its exact depth and course is variable. (4) The nasolacrimal duct system has been reported injured after rhinoplasty, most commonly affecting the nasolacrimal sac, beneath the medial canthal ligament, and the ductal ostium in the inferior meatus. (5) The nasolacrimal sac is most easily injured because it is not fully protected by the medial canthal ligament and can extend into the lacrimal crest. (6) Another study found transient obstruction of the nasolacrimal duct system at postoperative period one week (18% of patients) by measuring Tc-99m pertechneate instillation dacryoscintigraphy images. (7)
The nasal width should follow a graceful line from the brow to the tip, termed the brow-tip aesthetic. Discrepancies in width or contour will become readily evident on frontal view. Nasal bones too widely spaced may give the impression of telecanthus. The bony width of the bony sidewall of the nose should be approximately 75% of the distance of a normal alar base on frontal view. Deviations of the nose can be more readily appreciated by drawing a straight line from the midpoint between the brows to the upper lip and central incisors, provided there are no gross facial skeletal asymmetries. If there is facial deviation present, the nose may appear “straighter” if it is in line with the rest of the facial features.
Nasal bone geometry
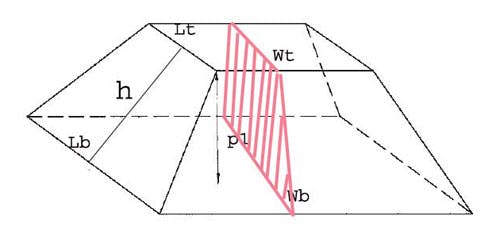
The nasal bones in shape and structure are comparable to a truncated pyramid, aka pyramidal frustum. It is inappropriate to conceptually think of osteotomies as just causing “nasal narrowing” without understanding the geometry of the nasal bones and the subsequent structural changes. A pyramidal frustum has a slant height (h), an overall height (p1), a bottom length (Lb) and top length (Lt), and a bottom width (Wb) and top width (Wt). (Figure 1) Similarly, the nasal bones can be subdivided into an overall height, slant height, dorsal width (corresponding to Wt) and ventral width (corresponds to Wb). The dorsal width is the width created by each nasal bone as it traverses from the midline horizontally, before it curves towards the face. The ventral width is the width created by the nasal bone and the nasal process of the maxilla as it traverses down to meet the horizontal face of the maxilla. Using the pyramidal frustum as a model for nasal bone dynamics, the type and location of the osteotomy will vary according to the desired aesthetic goal and underlying geometric proportions of the nasal bones.
Technique
There are two basic techniques for performing lateral osteotomies, sweeping and perforating. Sweeping osteotomies are performed with an osteotome in a continuous fashion. Typically the osteotomy is created in a high-low-high fashion. This translates to initially performing the osteotomy high along the pyriform aperture, low along the ascending maxilla, and then high again along superiorly along the nasal bones. For extra wide nasal bones, a low to high osteotomy will cause further narrowing of the facial width caudally. The osteotomy begins lower along the pyriform aperture and gently rises to the nasal bones superiorly. Extremely wide nasal bones, especially with a wide superior component, may benefit with an intermediate osteotomy.
The perforating osteotomy creates a series of small perforations along the nasal bones. Typically, a smaller osteotome (2.0 mm) will provide perforations along the ascending maxilla superiorly. The bones are then fractured in a controlled fashion. A perforating osteotomy may be performed percutaneously, especially superiorly. A 2.0 mm osteotome is tapped once through the soft tissue envelope of the nasal tissues. Controlled perforating fractures are then placed along the nasal bones. The perforated skin site will heal with inconsequential scarring even without suture placement, although there are divergent reports in the literature about this matter. (8,9) The percutaneous approach has been shown to have increased ecchymosis on the second day versus continuous internal techniques. (10)
Surgical opinion varies amongst whether lifting the periosteum off of the nasal bones is necessary. Proponents of periosteal elevation feel it decreases the amount of postoperative swelling by preventing periosteal tearing and subsequent bleeding.
In patients with previous osteotomies or comminuted nasal bones, periosteal elevating can be destabilizing to the underlying nasal bones. Kara, Kara, and Topaz found less ecchymosis and periorbital edema without periosteal undermining in a randomized trial; patients had undermining on one nasal side, and no undermining on the remaining half. (12)
Medial osteotomies are started at the junction of the upper lateral cartilage and nasal bones. A gentle fade of the osteotome towards the medial canthus ensures that the osteotome does not travel into the frontal bone and avoids a “rocker deformity”. Harshbarger and Sullivan found that nonfading or zero degree medial osteotomies resulted in contour irregularities and “rocker deformities” in seven out of eight noses in a cadaver. (13) However, when a slight 15 degree fade was incorporated, no contour irregularities or “rocker deformities” were encountered.
When performing the procedure through an endonasal approach, the surgical path of least resistance is often through an intercartilaginous incision. However, if the medial osteotomy is placed through an intercartilaginous incision, separation of the upper lateral cartilage from the septum is likely. This separation is prevented by placing the osteotome through a separate incision superior to the intercartilaginous incision, just at the junction of the upper lateral cartilage and the bony vault.
Becker, McLaughlin, Loevener and associates found that the use of smaller osteotomes created less intramucosal tearing when comparing 4 mm, 3 mm, and 2.5 mm guarded osteotomes. (1) Several authors have found that the thickness of the path of the lateral osteotomy is not more than 2.5 mm. (1, 14, 15)
Generally, speaking rasping should be performed prior to osteotomies. However, after osteotomies and infracture, the patient may have slight ridges and asymmetries along the nasal bone. These can be lessened by gentle rasping.
Wide Nasal Bones
Overly wide nasal bones may be managed by a variety of methods depending on the underlying anatomic cause. Most of the time, lateral and medial osteotomies are sufficient for narrowing of both the nasal and facial width of the nasal bones. In some instances, the medial osteotomy will provide a more controlled back fracture.
Excessively wide nasal width will sometimes require excision of a portion of medial nasal bone to allow for appropriate narrowing of the nasal bridge. (Figures 2-5) Without removal of the bone, it is sometimes difficult to achieve sufficient narrowing with medial osteotomies alone. Excision of the nasal bones is best performed with an external rhinoplasty approach. The soft tissue envelope is retracted so that the nasal width is seen along its entire length. An equal portion of nasal bone is removed with a nasal osteotome on each side and osteotomies are performed routinely after.
Overly wide nasal bones may be a result of overly wide facial width, which corresponds to an increased slant length. Usually, wide facial width will narrow appropriately with medial and lateral osteotomies. Rarely, overly wide facial width may require an intermediate osteotomy. (16, 17) The intermediate osteotomy is always performed first. An intermediate osteotomy will allow for appropriate narrowing of the nasal bones by causing an extra area of fracture along the slant height.
If the nasal bones are left wide after hump removal or require it for narrowing of the remainder of the nose, osteotomies can be performed medially and laterally. There are instances in which after hump removal, the nasal bone slant height is too short to provide sufficient narrowing to close the open roof deformity. (18) In these cases, dorsal augmentation with cartilage grafting may be needed to close the open roof deformity. When the surgeon plans to perform significant augmentation (i.e. with costal cartilage graft, alloplast, etc), osteotomies may not be necessary. Too much narrowing may create too narrow a pedestal for the dorsal graft to lie upon, and create unnatural shadows.
In cases in which the nasal bones are just slightly wider than ideal length, “defining osteotomies” can be performed. “Defining osteotomies” are lateral osteotomies without infracture of the nasal bones. (19) With time and contracture, the separation at the facial width will provide a slight degree of nasal narrowing and definition along the nasal bridge.
Crooked
The crooked nasal bony pyramid requires a cogitative approach from the surgeon. Most deviated nasal bones can be straightened by osteotomies performed as just discussed. There are specific instances when alternate maneuvers should be considered. If there is an asymmetric facial width, creating a discrepancy in slant height, a unilateral intermediate osteotomy should be considered. (Figure 6-9) If the slant height discrepancy is large, the surgeon should consider excision of nasal bone to provide a more equivalent slant height. An alternative maneuver is to rasp the nasal bones asymmetrically to provide better alignment in the slant height.
Persistently crooked nasal bones may be caused by the deviation at the ethmoid perpendicular plate. An osteotomy at the plate may allow for the deviation to be corrected. This is performed by placing the osteotome oblique to the line of the deviated nasal plate. The osteotome then displaces the nasal bony deviation to the contra lateral side with correction of the bony deformity. Jameson, Perry, and Ritter warn about the use of this technique in conjunction with dorsal hump removal due to destabilization of the dorsum. (20)
Cross-root osteotomies can also be performed. Cross root osteotomies mobilize the entire nasal pyramid and allow for alignment in cases of severe deviation. The osteotome path differs from a medial osteotomy in that the osteotomy is performed across the nasal bridge including the nasal dorsum. Cross-root osteotomies should only be used in select situations as improper usage can lead to dorsal instability and irregularities.
Overly narrowed
Overly narrowed nasal bones are typically a result of aggressive osteotomies from a prior surgeon. Several studies have demonstrated the consequences of narrowed nasal bones on airflow and airway obstruction. (21, 22) An overly narrowed nasal width may be widened with placement of spreader graft between the nasal bone and bony septum. After medial osteotomy, a space is created. Placement of a spreader graft will act as a doorstop, pushing the nasal bones wider. If the facial width is too narrow, placement of surgical packing may be needed to push the facial width wider. A silastic block may be carved for extremely narrowed noses and left in place for periods of up to 8 weeks. (23) Patients must be informed prior to surgery there will be increased nasal obstruction and pressure on the side of the packing or block placement. Byrne, Walsh, and Hilger described use of perforationg lateral osteotomies in an effort to widen the excessively narrow bony nasal pyramid. (24) They found that in a cadaver model, perforating lateral osteotomies had improved stability, better lateral repositioning, and less periosteal and mucosal tearing.
Unique Situations
A controversial issue is how wide does the surgeon place the osteotomy along the maxilla for lateral osteotomies. Each surgeon will have their own personal aesthetic on how much narrowing is desirable. As in all aspects of rhinoplasty, the osteotomy width must be balanced with the other features and characteristics of the nose. If the osteotomy takes place along the junction of the ascending maxilla and the face of the maxilla, the nasal bones are less likely to have a palpable bony step off. On the other hand, if the surgeon places the osteotome parallel to the face when performing osteotomies, a palpable step off will be minimized along the nasal bones. Bony step offs may be palpable but are typically not visible on exam.
If the surgeon narrows the ventral width too narrow, it may be narrower than dorsal width or provide an unnatural contour to the nasal bones. This will create the appearance of a “nasal indent” seen on the patient’s frontal view providing asymmetric shadows and a tell-tale sign of rhinoplasty.
Long faces and noses, will typically appear too thin with extra wide osteotomies creating a long narrow nose. Short noses may benefit from extra width in the osteotomy to give a narrower appearance to the nasal bridge and the illusion of length on frontal view.
The width of the nasal bones has effects on the appearance of facial structures. When the nasal bones are narrowed, the remainder of the face is wider in relation to the new nose. The illusion created is more prominence to the malar eminences and eyes. (18)
There are variations in nasal bone configuration which require specific attention. Nasal bones which are distinctly narrow at the nasion but widen as they progress caudally may require rasping at the cephalic portion of the bones so that the cephalic narrowing discrepancy is not so prominent.
Conclusion
The surgeon performing nasal width alignment should understand the complex three dimensional dynamics. Nasal models being developed may help further the understanding and planning of surgery in the future.
- Becker DB, McLaughlin RB, Loevner LA, Mang A. Clinical and Radiographic Rationale for Osteotome Selection. Plast Reconstr Surg 105: 1806, 2000.
- Citardi MJ, Hardeman S, Hollenbeak C, Kokoska M. Computer-aided assessment of bony nasal pyramid dimensions. Arch Otolaryngol Head Neck Surg 2000 126(8):979-84.
- Osguthorpe JD, Calcaterra TC. Nasolacrimal obstruction after maxillary sinus and rhinoplastic surgery. Arch Otolaryngol 1979 105(5):264-6.
- Thomas JR, Griner N. The relationship of lateral osteotomies in rhinoplasty to the lacrimal drainage system. Otolaryngol Head Neck Surg. 1986 94(3):362-7.
- Raut VV, Yung MW, Logan BM. Endoscopic dacrocystorhinostomy: anatomical approach. Rev Laryngol Otol Rhinol (Bord) 2000; 121(1):53-5.
- You ZH, Bell WH, Finn RA. Location of the nasolacrimal canal in relation to the high Le Fort I osteotomy. J Oral Maxillofac Surg 1992 50(10):1075-80.
- Uzun L. Ugur MB. Peksoy I. Cabuk M, Cinar F. The effect of lateral osteotomy of septorhinoplasty on nasolacrimal duct functions: a radionuclide imaging stuy. Am J Rhinol 2005 19(4):388-94.
- Hinton AE, Hung T, Daya H, O’Connell M. Visibility of puncture sites after external osteotomy in rhinoplastic surgery. Arch Facial Plast Surg. 2003 Sep-Oct;5(5):408-11.
- Gryskiewicz JM. Visible scars from percutaneous osteotomies.
Plast Reconstr Surg. 2005 Nov;116(6):1771-5. - Yucel OT. Which Type of Osteotomy for Edema and Ecchymosis: External or Internal? Ann Plast Surg. 2005 Dec;55(6):587-590
- Gryskiewicz JM, Gryskiewicz KM. Nasal osteotomies: a clinical comparison of the perforating methods versus the continuous technique.
Plast Reconstr Surg. 2004 Apr 15;113(5):1445-56; discussion 1457-8. - Kara CO, Kara IG, Topuz B. Does creating a subperiosteal tunnel influence the periorbital edema and ecchymosis in rhinoplasty? J Oral Maxillofac Surg. 2005 Aug;63(8):1088-90.
- Harshbarger RJ, Sullivan PK. The Optimal Medial Osteotomy: A Study of Nasal Bone Thickness and Fracture Patterns. Plast Reconstr Surg 108: 2114, 2001.
- Harshbarger RJ, Sullivan PK. Lateral nasal osteotomies: implications of bony thickness on fracture patterns.
Ann Plast Surg. 1999 Apr;42(4):365-70; discussion 370-1. - Kuran I, Ozcan H, Usta A, Bas L. Comparison of four different types of osteotomes for lateral osteotomy: a cadaver study.
Aesthetic Plast Surg. 1996 Jul-Aug;20(4):323-6. - Harris MO, Baker SR. Management of the wide nasal dorsum. Arch Facial Plast Surg. 2004 Jan-Feb;6(1):41-8.
- Westreich RW, Lawson W. Perforating double lateral osteotomy.
Arch Facial Plast Surg. 2005 Jul-Aug;7(4):257-60. - Sheen JH. Aesthetic Rhinoplasty. St. Louis, MO: CV Mosby, 1978
- Norman Pastorek. Personal Communication 2006.
- Jameson JJ, Perry AD, Ritter EF. High Septal Osteotomy in Rhinoplasty for the Deviated Nose. Ann Plast Surg. 2006 Jan;56(1):40-45.
- Grymer LF, Gregers-Petersen C, Baymler Pedersen H. Influence of lateral osteotomies in the dimensions of the nasal cavity.
Laryngoscope. 1999 Jun;109(6):936-8. - Guyuron B. Nasal osteotomy and airway changes.
Plast Reconstr Surg. 1998 Sep;102(3):856-60; discussion 861-3. - Dean Toriumi. Personal Communication 2003
- Bryne PJ, Walsh WE, Hilger PA. The use of “inside-out” lateral osteotomies to improve outcome in rhinoplasty. Arch Facial Plast Surg. 2003 5(3):252-5.
The pyramidal frustrum serves as a geometric model for analyzing nasal bone discrepancies. Lt= dorsal length, Lb=ventral length, p1=overall height, h=slant height, Wt=dorsal width, Wb=ventral width
“The nose should fit the face”
A strong jawline would suggest a stronger nose.
